"please keep me updated about oximeters "
Sleep Apnea Forum Bringing Power to the Patient
New? Free Sign Up
Then check our Welcome Center to a Community Caring about Sleep Apnea diagnosis and Sleep Apnea treatment:
CPAP machines, Sleep Apnea surgery and dental appliances.
CPAP Supplies
Latest Activity
child 9 years old, AHI = 4.4, is that good? Problem? Whats the range?
Our behaviorally challenged middle child was sent for a sleep study to rule out sleep disorders. His special ed. teacher and the pediatrician had suspected seizures or something may be disrupting sleep. But we were all surprised by the results. The report recommended taking him to an ENT for evaluation of his upper airway. "The patient was noted to have central sleep apnea with AHI=4.4, the lowest oxygen saturation was 93%." Go figure, all the brainwave results were unremarkable. Can anybody help us understand these numbers?
Views: 743
Replies to This Discussion
-
Permalink Reply by Jeanne Lyon on
-
There is none listed in this report. The column marked "Avg." under End Tidal Carbon Dioxide Distribution lists 45 for REM, 45 for NREM and 45 for Total(TIB). The Sleep Architecture chart has a total sleep time listed of 381.5min. Sorry, maybe the information you seek is there, but I dont know how to find it. There's a Night Hypnogram graph on another page which shows a line for ETCO2mmHg, and it looks like its at 45 across the span from 10:25pm to 6:00am, with a few dips at 12am and 1:30am.
My dear husband thinks the boy has brain stem issues, and cardio-pulmonary may be secondary to that. Our goal will be to have good enough information that will assist us to be taken seriously at the doctors' office, and hopefully find a way to help our son out of his bizarre existence and reach his full potential. He is SO smart, but only able to do very little.
-
-
DH can scan this later today, he'll have to go to his office to use his scanner. Thank you! We got an ENT appointment for Oct 27, then a regular ped's appointment the next day.
-
-
Here is a scan of the report.
- Attachments:
-
-
 Arthur's Sleep Study.pdf, 159 KB
Arthur's Sleep Study.pdf, 159 KB
-
-
Permalink Reply by James Skinner on
-
Personally I would highly recommend getting your child off Prozac if you want him to be able to sleep. SSRIs are notorious for affecting peoples ability to sleep. Why is he on Prozac? If its anxiety, the centrals might be the cause. Follow up on those centrals to try and figure out why they are happening.
-
Permalink Reply by 99 on
-
i am not a doctor or health proi suggest that should your son become hospitalizd (i hope he not hospitazed) for whatever reason EG a brocken arm etc that you put the problem to you doctor or hospital staff to include what you are seeking to secure before time to get the treatment at the same time
-
-
I don't know what AHI is. Could someone please explain?
How many Central sleep apnea events per hour does your son have (according to the overnight sleep study)?
I do know what Central Sleep Apnea is, though. There is a prolonged pause at the end of an exhale, before starting the next inhale, i.e., a delay in the signal to take the next breath reaching the lungs, either due to some fault in the brain stem, or some interruption in the signal to breathe on the way from the brain stem to the lungs.
My sleep neurologist explained to me that means that each time there is a prolonged pause, i.e. a central apnea event, the brain neurologically awakens the person, even though the person seems to be sound asleep and believes that he or she was asleep.
This means that when a person wakes up in the morning, the person with central sleep apnea will have had interrupted sleep all night and not be aware of it. In my case, I had 21 Central sleep apnea events per hour. I though I was sound asleep, and my obstructive sleep apneas had been corrected with an oral appliance (my lower jaw is too far back, big tongue flops back when I sleep - not the usual cause of obstructive sleep apnea), I was still exhausted during the day, because I was neurologically awakening all night long and had no REM sleep (deep sleep).
That would certainly affect the behavior of a child of any age.
The obstructive can have many causes. There could be a deviated septum, a polyp in a nostril, soft tissue issues in the mouth, etc., etc. The ENT is a very good idea.
Obstructive can masquerade at Central, or there can be true Central. If a CPAP machine is used, but after - how many months was it? who posted information on this? a cerain amount of time, an overnight sleep study with the CPAP and the face mask or nasal mask or nasal pillows shows good correction of Obstructive Sleep Apnea (OSA), but that the Central Sleep Apnea (CSA) events are still there, then there probably is true Central apnea, also.
Your son can have both. I have both. I feel much better on a special machine for Central sleep apnea that, in my case with the oral appliance for the jaw problem, also corrects the Obstructive, and I am finally able to get on with my life during the day.
-
Permalink Reply by RockRpsgt on
-
AHI=apnea+hypopnea index. This is the average number of apneas and hypopneas per hour.
Vicki I am so proud of you.
-
Permalink Reply by terri on
-
My 9 yr old grandson is also behaviorally challenged but it has never been suggested that he may have a sleep disorder. He has a tendency to pause between breaths ie; breath, hold his breath for a few seconds, breath again. while he is awake. His ped. says this is normal. Does anyone know if there could be a correlation between this and central apnea?
-
-
I am not a medical professional. Just a long term sufferer of central sleep apnea, brain dysfunction (possibly brain stem), seizure disorder, SSRI user and devoted online researcher of these conditions.
I am very concerned about the long term effects of the Prozec. A 9 yo has a very immature brain and interrupting its function with an SSRI is scary in my understanding. I would find a neuro-psychiatrist to do an extensive QEEG study, especially P300 to determine how his brain is handling information. He might be responsive to QEEG based neuro-therapy. There also may be more natural ways of moderating his neurotransmitters besides an SSRI.
I'd keep him away from diet sweeteners, MSG, caffeine, etc. Blood work to determine his B-12 and folate levels would be interesting. A fasting glucose test would too. Heavy metals?? Not the standard test for heavy metals but tests done by a physician who has a strong understanding of heavy metals. I do not fully understand the issues but my physician tried to explain them to me. He said that standard heavy metals levels per health industry standards is much higher than occupational heavy metals limits per OSHA. .
Here in Boise, we have a cluster of learning disabled from autism to Down's in the children of the workers at Micron Technology, a computer memory manufacturer. The last I heard, they estimate the rate is 12 times higher than in a normal population. They suspect heavy metals may have effected the parents' and got genetically passed to the children. They are just starting to investigate this cluster. There is already anecdotal data to suggest that mothers who had more than 5 amalgam fillings during the first two trimesters of their pregnancy has a higher risk of learning disabilities in the child from that pregnancy.
I don't want to be an alarmist. But we do want to find answers and understand how to care for these children.
BTW, Has he ever had a concussion or high fever? Was his birth uneventful or was labor excessively long and delayed?
-
-
Thank you everybody here for the discussion! At least now we know something about sleep study reports. I work 12hour day shifts, I have been away working for a few days and have not had the chance to check my emails very well. Is there anything we should ask the ENT when we have our appointment on Tuesday 10/27?
-
-
What is POPE?
Mollete said:I think that before you get there, you have to be sure that the central events are, in fact, central events. Clearly, none of them are >20 seconds: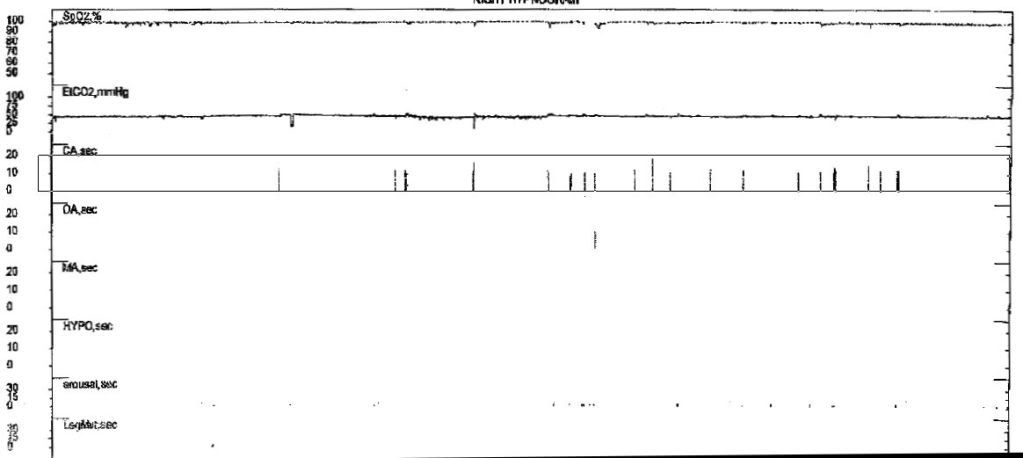
Only 2 of the central apneas (and the lone obstructive apnea) MAY have associated desaturations (although this parameter is not listed on the report, which makes this a "rogue" study). So if the remaining centrals have no associated arousals, or are post-arousal in nature, then the AHI is not 4.4, but 0.6.
This is crucial information, because if the ENT surgeon says, "Well, your son's tonsils look OK, but that AHI of 4.4 is higher than our standard of 3.0 (or whatever value that is higher than 0.6) so we're going to go ahead and cut anyway", you can say "OK, hold your horses there, Jim Bowie, we need to think about this. Let's talk about POPE".
mollete

- ‹ Previous
- 1
- 2
- Next ›
© 2026 Created by The SleepGuide Crew.
Powered by
![]()